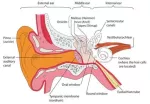
Otitis media (OM) is any inflammation of the middle ear (see the images below), without reference to etiology or pathogenesis. It is very common in children.
There are several subtypes of OM, as follows:
- Acute OM (AOM)
- OM with effusion (OME)
- Chronic suppurative OM
- Adhesive OM
Signs and symptoms
AOM implies rapid onset of disease associated with one or more of the following symptoms:
- Otalgia
- Otorrhea
- Headache
- Fever
- Irritability
- Loss of appetite
- Vomiting
- Diarrhea
OME often follows an episode of AOM. Symptoms that may be indicative of OME include the following:
- Hearing loss
- Tinnitus
- Vertigo
- Otalgia
Chronic suppurative otitis media is a persistent ear infection that results in tearing or perforation of the eardrum.
Adhesive otitis media occurs when a thin retracted ear drum becomes sucked into the middle ear space and stuck.
Diagnosis
OME does not benefit from antibiotic treatment. Therefore, it is critical for clinicians to be able to distinguish normal middle ear status from OME or AOM. Doing so will avoid unnecessary use of antibiotics, which leads to increased adverse effects of medication and facilitates the development of antimicrobial resistance.
Management
Most cases of AOM improve spontaneously. Cases that require treatment may be managed with antibiotics and analgesics or with observation alone.
Guidelines from American Academy of Pediatrics
In February 2013, the American Academy of Pediatrics (AAP) and the American Academy of Family Physicians (AAFP) released updated guidelines for the diagnosis and management of AOM, including recurrent AOM, in children aged 6 months through 12 years. The recommendations offer more rigorous diagnostic criteria to reduce unnecessary antibiotic use.
According to the guidelines, management of AOM should include an assessment of pain. Analgesics, particularly acetaminophen and ibuprofen, should be used to treat pain whether antibiotic therapy is or is not prescribed.
Recommendations for prescribing antibiotics include the following:
- Antibiotics should be prescribed for bilateral or unilateral AOM in children aged at least 6 months with severe signs or symptoms (moderate or severe otalgia, otalgia for 48 hours or longer, or temperature 39°C or higher) and for nonsevere, bilateral AOM in children aged 6 to 23 months
- On the basis of joint decision-making with the parents, unilateral, nonsevere AOM in children aged 6-23 months or nonsevere AOM in older children may be managed either with antibiotics or with close follow-up and withholding antibiotics unless the child worsens or does not improve within 48-72 hours of symptom onset
- Amoxicillin is the antibiotic of choice unless the child received it within 30 days, has concurrent purulent conjunctivitis, or is allergic to penicillin; in these cases, clinicians should prescribe an antibiotic with additional beta-lactamase coverage.